In a newly published case series, Drs. Arjun Desai, Mudit Tyagi, Brijesh Takkar, and others from LVPEI described the efficacy of fibrin glue as a tamponade in the surgical management of complex rhegmatogenous retinal detachment.
The retina, a delicate, inner layer of tissue and light-sensitive cells, is susceptible to physical forces that can peel it off the back of the eye, resulting in a set of blinding conditions called retinal detachments (RD). Rhegmatogenous retinal detachment (RRD)— from the Greek word, Rhegma, or break—is when a tear or break in the retinal tissue causes fluid (vitreous) to leak in and accumulate between the retina and an underlying layer of retina-nourishing tissue, the retinal pigment epithelium. This fluid accumulation builds up pressure and pushes against the retina, detaching it. Complex RRDs are when many things go wrong: a large retinal break, abnormal epiretinal membranes, infection, or more. Treatment involves complex surgery for sealing the breaks in the retina and is fraught with failures and complications.
A ‘tamponade,’ usually a gas or silicone oil, is often injected into the eye to keep the retinal tear from reopening and the repaired tissue reattaches healthily. But both gas and oil tamponades are sub-optimal and inadequate at keeping the torn retinal tissue together in complex RRDs. What is the solution? Fibrin glue is a biological adhesive made from fibrinogen and thrombin; proteins involved in blood clotting. The glue is non-toxic and gets gradually absorbed by ocular tissues as these proteins are naturally present in our bodies. Fibrin glue has shown promising results as an alternative tamponade agent for simple RRDs and for closing macular holes. But will it be equally effective in complex RRD cases?
In a new paper published in the Journal of Vitreoretinal Diseases, Drs. Arjun Desai, Mudit Tyagi, Brijesh Takkar, and others from LVPEI describe five complex RRD cases where they used fibrin glue as a tamponade. Along with the RRD, each patient had other complications that increased the risk of glaucoma upon intervention, such as aphakia (no natural lens), aniridia (no iris tissue) or pre-existing glaucoma (abnormal intraocular pressure). The patients in all five cases underwent vitrectomy (to remove the vitreous) and laser retinopexy (to seal the tear), performed by the same surgeon. Fibrin glue was injected into the eye to seal any breaks in the retina.
In all five cases, fibrin glue worked safely and efficaciously as the sole or supplementary tamponade agent. It effectively sealed the break and stopped ocular fluid in the present case series, attaining a successful attachment in all patients, while minimizing the chances of surgical failure and damage to other ocular tissues, a major risk in conventional surgery.
‘Fibrin glue provides extra support in sealing severely torn retinal tissue and can work both in isolation as well as an adjunctive tamponade,’ remarks Dr. Brijesh Takkar, an ophthalmologist at LVPEI and the corresponding author of this paper. ‘We found it specifically useful in cases where conventional surgery may have led to complications, like corneal damage and eye pressure rise, or would have resulted in failure due to thick fluid and blood below the retina. The best part is that fibrin glue is a physiological product, and hence devoid of complications.’
Citation
Desai, A., Bhopalka, A. K., Tyagi, M., Sharma, S. V., & Takkar, B. (2024). Glue-Assisted Retinopexy for Retinal Detachments Study Report 2: Fibrin Glue as a Surgical Adjunct in Complex Rhegmatogenous Retinal Detachment. Journal of Vitreoretinal Diseases, 8(4), 435–441. https://doi.org/10.1177/24741264241247623
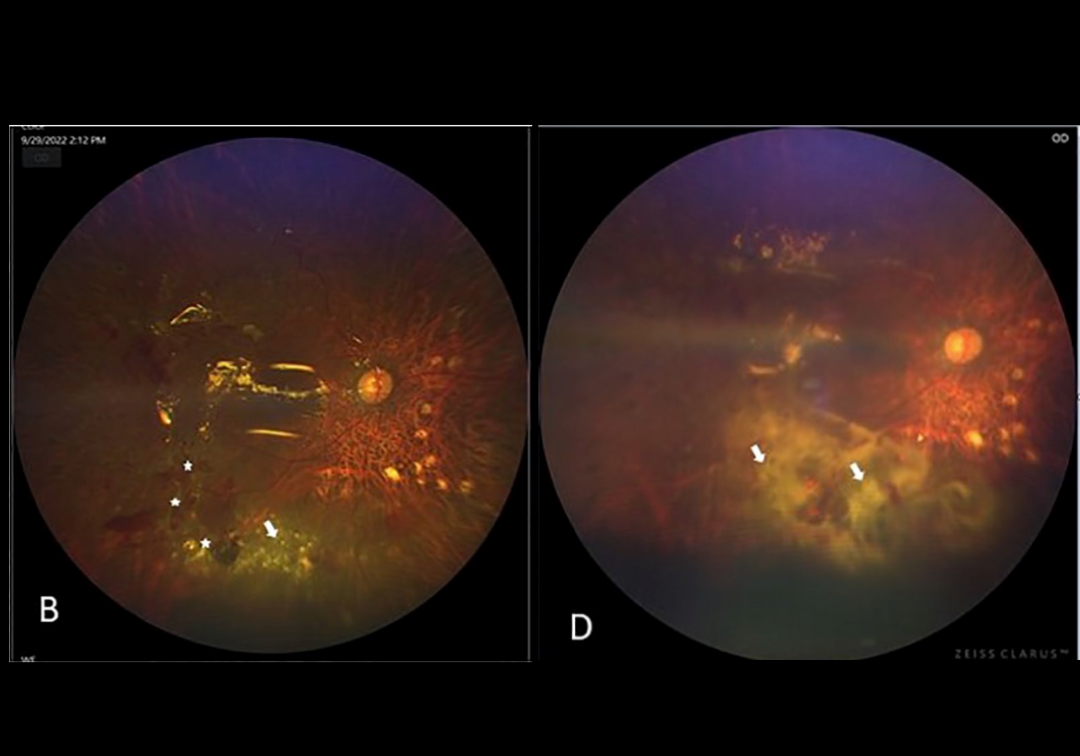
Photo credit: Fundus photographs with fibrin glue application (white arrows), Desai et al.